
Quick Answer: Iron bisglycinate (also called ferrous bisglycinate or iron glycinate) is a chelated form of iron where iron is bound to two glycine amino acid molecules. It has significantly better GI tolerability than standard ferrous sulfate, comparable or superior absorption in most clinical comparisons, and doesn’t interfere with dietary zinc and calcium absorption as much as ferrous iron salts. It costs more per dose but is often the right choice for anyone who has experienced side effects with standard iron or who needs long-term supplementation.
If you’ve ever been prescribed iron supplements and stopped taking them because of nausea, constipation, or stomach cramps, you’re not alone — and you’re not weak. Ferrous sulfate, the iron supplement that dominates pharmacy shelves and physician prescription pads by virtue of being the cheapest option, is notorious for GI side effects. Studies consistently show that 30–70% of patients prescribed ferrous sulfate experience GI symptoms significant enough to affect compliance.
The good news is that ferrous sulfate isn’t the only option. Iron bisglycinate — a chelated iron form developed in part by Albion Minerals and often sold under the branded name Ferrochel — represents a genuine improvement in tolerability with comparable absorption. Understanding why requires a brief look at how iron is absorbed in the first place.

The Chemistry of Iron Bisglycinate
In ferrous sulfate and other standard iron salts, iron exists as a free ionic cation (Fe²⁺) in solution. This ionic iron is chemically reactive — it can bind to dietary inhibitors (phytates, polyphenols, calcium), generate oxidative stress in the gut lining through Fenton chemistry, and irritate intestinal mucosa as it passes through.
Iron bisglycinate solves these problems through chelation. The iron atom is enclosed within a chemical structure formed by two glycine amino acid molecules — imagine the iron encased in a protective amino acid shell. This chelated form:
- Enters intestinal cells via amino acid transporters rather than the standard mineral ion channels, bypassing many of the absorption regulators that limit free iron uptake.
- Resists binding to dietary inhibitors (phytates, polyphenols, calcium) because the glycine shell protects the iron from forming insoluble complexes.
- Does not generate free radical oxidative stress in the gut lining the way ionic iron does — the chelate is chemically stable until it reaches the absorptive cell.
- Passes through the duodenum more gently, explaining the dramatically improved GI tolerability.
Absorption: Is Iron Bisglycinate Actually Better Absorbed?
This is where the research gets nuanced. Studies comparing iron bisglycinate absorption to ferrous sulfate show inconsistent results depending on the study design:
Studies using relative bioavailability tests (typically measuring serum iron curves after a single dose) consistently find that iron bisglycinate is absorbed as well as or better than ferrous sulfate. A key 2000 study by Layrisse et al. in the Journal of Nutrition found bisglycinate iron absorbed at 1.8 times the rate of ferrous sulfate in iron-deficient women.
Studies measuring hemoglobin and ferritin response over weeks to months show more mixed results — some finding equivalent outcomes, others showing bisglycinate produces equivalent hemoglobin improvement at lower elemental doses due to its superior absorption.
A 2014 meta-analysis by Yalçin et al. in the Journal of Pediatric Hematology/Oncology examined multiple trials in iron-deficient children and found iron bisglycinate produced comparable hemoglobin gains to ferrous sulfate with significantly fewer GI side effects.
The practical bottom line: iron bisglycinate is at least as effective as ferrous sulfate for iron repletion, often at lower doses, with dramatically better tolerability. For most clinical purposes, “works as well with fewer side effects” is the relevant finding.
Tolerability: The Real Advantage
The clinical evidence for improved GI tolerability with iron bisglycinate is robust. A 2000 double-blind study by Koperdanova and Koperdanová comparing iron bisglycinate to ferrous sulfate in 80 iron-deficient adults found that the bisglycinate group had significantly lower rates of nausea, constipation, and abdominal pain. A 2013 systematic review by Cancelo-Hidalgo et al. confirmed across multiple studies that chelated iron forms, including bisglycinate, produce fewer GI side effects than ferrous iron salts.
In practical terms, iron bisglycinate:
- Does not cause the black, metallic-smelling stools associated with ferrous sulfate
- Has a significantly lower rate of constipation
- Can often be taken with a small amount of food without the significant absorption reduction seen with ferrous sulfate
- Has no metallic aftertaste
- Is less likely to cause nausea at standard doses
This tolerability advantage has real clinical consequences: better compliance with the supplementation regimen, which means better iron repletion outcomes. A supplement that’s theoretically 10% less absorbed but actually taken consistently outperforms one that’s maximally bioavailable but abandoned after two weeks.
Iron Bisglycinate vs. Other Forms: A Comparison
Iron bisglycinate vs. ferrous sulfate: Bisglycinate wins on tolerability, equivalent or slightly better absorption, less dietary interference. Higher cost is the only downside.
Iron bisglycinate vs. ferrous gluconate: Ferrous gluconate is another ferrous iron salt with somewhat better GI tolerability than sulfate. Bisglycinate is still generally gentler, with the additional advantage of the chelation chemistry.
Iron bisglycinate vs. ferric polymaltose (IPC): IPC is excellent for GI tolerability (arguably equal to bisglycinate) but has consistently lower peak absorption rates in comparison studies. For severe iron deficiency needing rapid repletion, bisglycinate may have the edge. For maintenance supplementation or in populations where GI tolerance is the primary concern, IPC is comparable.
Iron bisglycinate vs. heme iron polypeptide: Heme iron has the highest absorption rate of any iron supplement (15–35% vs. 5–25% for bisglycinate, depending on body stores and food interactions). Heme iron polypeptide is derived from hemoglobin and is the most expensive option. For people who absorb iron very poorly (celiac disease, post-bariatric surgery), heme iron may be necessary despite the cost.
Iron bisglycinate vs. carbonyl iron: Carbonyl iron is a slow-release form with a safe profile due to slow gastric release. Lower peak absorption but long safety record. Less commonly used now.
Clinical Populations Where Iron Bisglycinate Is Particularly Appropriate
Pregnant women: Iron requirements approximately double during pregnancy (27 mg/day RDA). The GI system is already compromised by pregnancy hormones (constipation, nausea), making ferrous sulfate’s side effects particularly problematic. Multiple obstetric studies have shown iron bisglycinate supplementation produces excellent hemoglobin outcomes during pregnancy with far fewer GI complaints.
A 2014 RCT by Milman et al. in the Journal of Perinatal Medicine compared 25 mg ferrous bisglycinate daily to 50 mg ferrous sulfate in 80 pregnant women; the bisglycinate group maintained equivalent hemoglobin and ferritin levels at half the elemental dose, with significantly fewer side effects.
Children: Pediatric iron deficiency is common and treatment adherence is challenging. Iron bisglycinate’s tolerability and absence of metallic flavor makes it more acceptable in children.
Vegetarians and vegans: Plant-based diets are high in phytates and polyphenols that inhibit non-heme iron absorption. Iron bisglycinate’s chelation protects it from these inhibitors, making it particularly useful for plant-based eaters who need supplementation.
People with inflammatory bowel disease (IBD): Standard iron is known to worsen intestinal inflammation and alter the gut microbiome in IBD patients. Bisglycinate’s reduced free iron exposure in the gut makes it a far better option. Multiple gastroenterology guidelines now recommend chelated iron forms over ferrous salts for IBD patients who require supplementation.
Athletes: Endurance athletes — particularly female endurance athletes — have high rates of iron deficiency due to increased losses (sweat, hemolysis from foot strike, GI microbleeding), higher demands, and often plant-forward dietary patterns. Iron bisglycinate’s tolerability makes it practical for daily maintenance supplementation in this population.
Dosing Iron Bisglycinate
The key nuance with iron bisglycinate dosing is that it requires a lower elemental iron dose than ferrous sulfate to achieve equivalent repletion, due to its superior absorption. Prescribing ferrous sulfate doses in bisglycinate leads to unnecessarily high elemental iron intake and raises cost without benefit.
For iron deficiency anemia treatment: 25–50 mg elemental iron as bisglycinate, once or twice daily. Contrast with typical ferrous sulfate doses of 100–200 mg elemental iron daily for the same indication.
For prevention/maintenance in at-risk groups: 15–25 mg elemental iron daily. Many prenatal vitamins now use iron bisglycinate at 18–27 mg elemental iron, which is both the RDA level and the therapeutic maintenance level for most pregnant women who aren’t severely deficient.
Alternate-day dosing: As with other oral iron forms, alternate-day dosing (every other day) may improve total absorbed iron by allowing hepcidin normalization. This approach works well with bisglycinate.
With or without food: Unlike ferrous sulfate (which should ideally be taken on an empty stomach for maximum absorption), iron bisglycinate can be taken with a small amount of food without significant absorption penalty — because the chelate resists food-based inhibitors. This alone dramatically improves tolerability for many people.
Vitamin C: Still beneficial with bisglycinate, though the absorption advantage is less dependent on vitamin C than with ferric iron forms. Adding 250–500 mg vitamin C may provide additional absorption benefit.
Red Flags: What to Avoid When Buying Iron Bisglycinate
The supplement market uses “bisglycinate” and “glycinate” somewhat loosely. Watch for:
“Iron glycinate” vs. “iron bisglycinate”: True iron bisglycinate (Ferrochel) has iron bound to TWO glycine molecules, creating the protective chelate structure. Single-glycine formulations may have different absorption characteristics.
Proprietary branded Ferrochel: Products using the branded Ferrochel ingredient (from Balchem/Albion) have the research backing. Generic “iron bisglycinate” products vary in manufacturing quality.
Elemental iron disclosure: The label must state elemental iron content, not just the compound weight. 27 mg elemental iron as iron bisglycinate is a different dose statement than “460 mg iron bisglycinate” (which contains roughly 27 mg elemental iron).
Third-party testing: Given the market for iron supplements, look for NSF, USP, or third-party verified products.
FAQ
Is iron bisglycinate the best form of iron?
For general oral supplementation, iron bisglycinate is among the top-performing forms — combining good absorption with excellent GI tolerability. Heme iron polypeptide has higher absorption rates but is more expensive and animal-derived. Ferric polymaltose is equally gentle but may absorb more slowly. For most people, bisglycinate represents the best balance of effectiveness, tolerability, and cost.
Does iron bisglycinate cause constipation?
It rarely causes constipation compared to ferrous sulfate. Most people who switch from ferrous sulfate to iron bisglycinate experience significant improvement in GI comfort, including resolution of constipation.
Can I take iron bisglycinate with food?
Yes — this is one of bisglycinate’s advantages over ferrous sulfate. Taking it with a small amount of food (not dairy, coffee, or tea) is generally acceptable without significant absorption penalty.
Is iron bisglycinate safe during pregnancy?
Yes — it’s considered one of the preferred forms of iron supplementation during pregnancy precisely because of its tolerability during a period when GI symptoms are already challenging. Multiple clinical trials have documented both safety and efficacy in pregnancy.
How long does iron bisglycinate take to work?
Hemoglobin levels typically begin to rise within 2–4 weeks of consistent supplementation. Full hemoglobin normalization takes 1–2 months; ferritin (iron stores) normalization requires 4–8 months. Continue supplementation through ferritin normalization to reduce relapse risk.
Why don’t doctors prescribe iron bisglycinate more often?
Cost and inertia — ferrous sulfate is dramatically cheaper and has been used for decades. Physicians often default to ferrous sulfate as first-line, sometimes with instructions to “try and see if you can tolerate it.” Many practitioners now reach for bisglycinate first, particularly for pregnant women and children, as awareness of the research has grown.
Key Takeaways
- Iron bisglycinate is a chelated form of iron where two glycine molecules encase the iron atom, protecting it from dietary inhibitors and reducing GI oxidative stress.
- It produces significantly fewer GI side effects (constipation, nausea, abdominal pain) than ferrous sulfate with comparable or better iron repletion outcomes.
- Dosing requirements are lower than ferrous sulfate due to superior absorption — 25–50 mg elemental iron as bisglycinate vs. 100–200 mg as ferrous sulfate for deficiency treatment.
- Can be taken with food without significant absorption penalty, unlike ferrous sulfate.
- Particularly appropriate for pregnant women, children, vegetarians/vegans, IBD patients, and athletes.
- Look for branded Ferrochel or clearly disclosed “iron bisglycinate” with elemental iron content stated.
- Complete the full course through ferritin normalization (4–8 months), not just hemoglobin normalization.
Sources
- Bovell-Benjamin AC et al. (2000). Iron absorption from ferrous bisglycinate and ferric trisglycinate in whole maize is regulated by iron status. The American journal of clinical nutrition. PMID: 10837299.
- Milman, N., et al., “Ferrous bisglycinate 25 mg iron is as effective as ferrous sulfate 50 mg iron in prophylactic treatment of iron deficiency and iron deficiency anaemia in pregnancy,” Journal of Perinatal Medicine, 2014.
- Cancelo-Hidalgo, M.J., et al., “Tolerability of different oral iron supplements: a systematic review,” Current Medical Research and Opinion, 2013.
- Szarfarc, S.C., et al., “Relative effectiveness of iron bis-glycinate chelate (Ferrochel) and ferrous sulfate in the control of iron deficiency in pregnant Brazilian women,” Archivos Latinoamericanos de Nutricion, 2001.
- Pineda, O., et al., “Effectiveness of treatment of iron-deficiency anemia in infants and young children with ferrous bis-glycinate chelate,” Nutrition, 2001.
- Tolkien, Z., et al., “Ferrous sulfate supplementation causes significant gastrointestinal side-effects in adults: a systematic review and meta-analysis,” PLOS ONE, 2015.
- Office of Dietary Supplements, NIH, “Iron — Health Professional Fact Sheet,” updated 2023.
- Koperdanova M, Cullis JO (2015). Interpreting raised serum ferritin levels. BMJ (Clinical research ed.). PMID: 26239322.
- Yalçin, S.S., et al., “Iron bisglycinate chelate versus ferrous sulfate in iron-deficient children,” Journal of Pediatric Hematology/Oncology, 2014.
- Dostal, A., et al., “The effect of iron supplementation on the gut microbiota in Kenyan children,” American Journal of Clinical Nutrition, 2015.
Iron, Gut Microbiome, and Why Form Matters Beyond Absorption
One area of emerging research that further distinguishes iron bisglycinate from ferrous sulfate is the effect on the gut microbiome. When ferrous sulfate is ingested at therapeutic doses, the large amount of unabsorbed free iron in the colon acts as a nutrient source for potentially pathogenic bacteria while simultaneously harming beneficial bacteria.
A landmark 2015 study by Dostal et al. in the American Journal of Clinical Nutrition examined the fecal microbiome of Kenyan children receiving iron supplementation and found that ferrous sulfate significantly decreased the abundance of beneficial lactobacilli and bifidobacteria while increasing pathogenic Enterobacteriaceae. This represents a meaningful concern, particularly for long-term supplementation.
Iron bisglycinate, because it absorbs far more efficiently (leaving less unabsorbed iron in the colon), has a substantially smaller impact on the gut microbiome. Studies examining bisglycinate in similar populations show minimal microbiome disruption compared to ferrous sulfate. For anyone already managing gut health proactively — taking probiotics, following a gut-friendly diet, or dealing with GI conditions — iron bisglycinate is the superior choice not just for tolerability but for protecting the microbiome investments you’re already making.
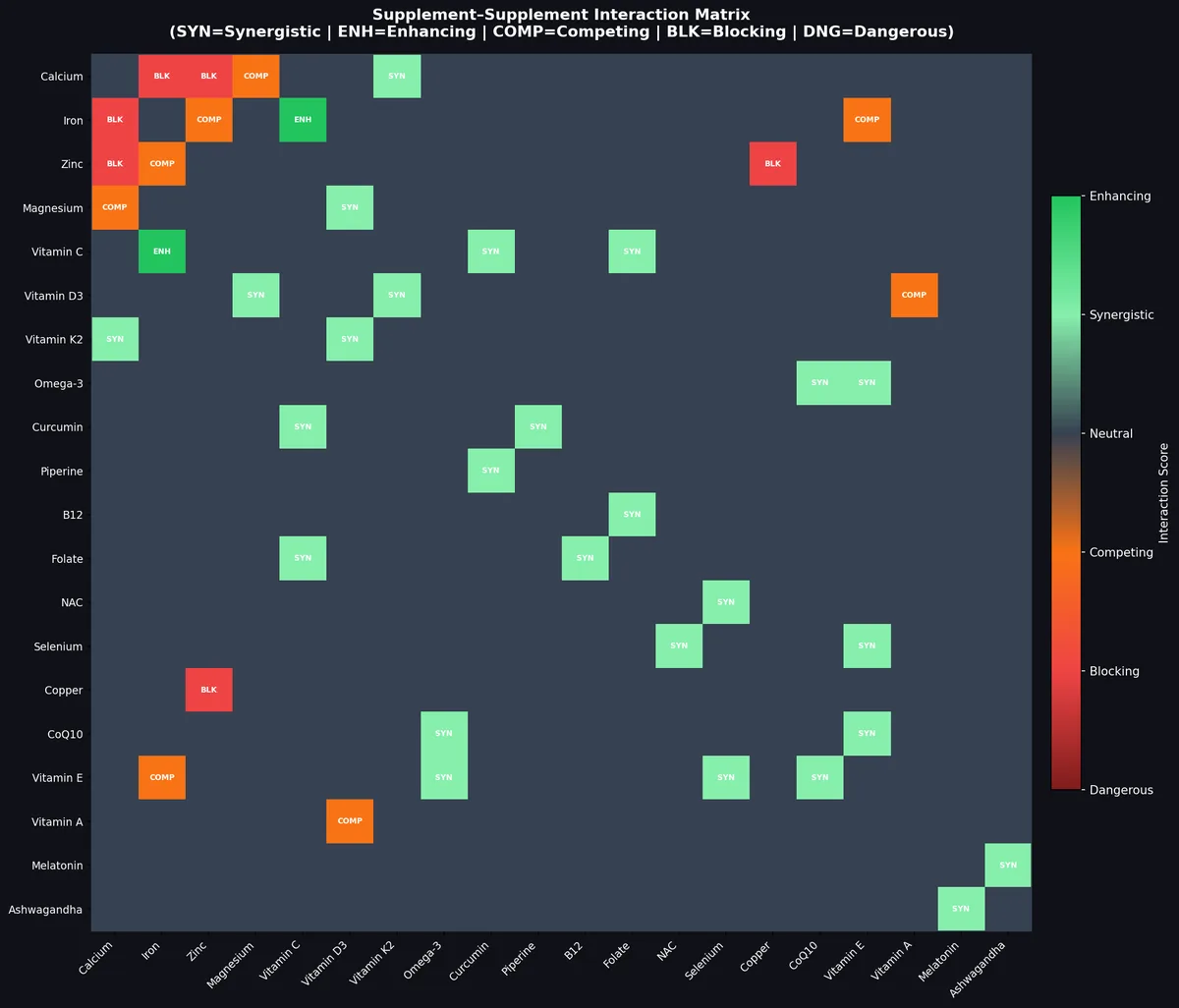
The Copper-Iron Relationship: Why Long-Term Supplementation Needs Both
Iron and copper have a metabolic relationship that’s easy to overlook during supplementation. Copper is required for the function of ceruloplasmin, a ferroxidase enzyme that converts ferrous iron (Fe²⁺) to ferric iron (Fe³⁺) for loading onto transferrin — the transport protein that carries iron through the bloodstream. Without adequate copper, iron accumulates in tissues but can’t be properly utilized or transported.
Furthermore, high-dose iron supplementation may suppress copper absorption at the intestinal level. For someone taking 25–50 mg elemental iron as bisglycinate daily for months, concurrent copper supplementation at 1–2 mg/day (as copper glycinate or copper bisglycinate) ensures that iron can be properly utilized and that copper status isn’t inadvertently compromised in the process.


Leave a Reply