Most supplement stacks are assembled backwards. People add supplements one at a time based on whatever health goal they’re currently chasing — sleep, energy, immunity — without ever mapping how those supplements interact with each other. The result is often a pile of capsules that partially cancel each other out.
Some combinations are powerfully synergistic. Curcumin + piperine increases curcumin bioavailability by around 2,000% in the classic Shoba 1998 human study. Vitamin D3 + K2 together do something neither achieves alone. Others are silent conflicts: high-dose calcium taken with iron-containing meals has been shown in controlled studies to reduce non-heme iron absorption by roughly 50–60% at the doses most relevant to supplement users. Taken daily, that can contribute to iron deficiency in people who think they’re supplementing iron adequately.
This database is the reference you need before assembling any serious stack.
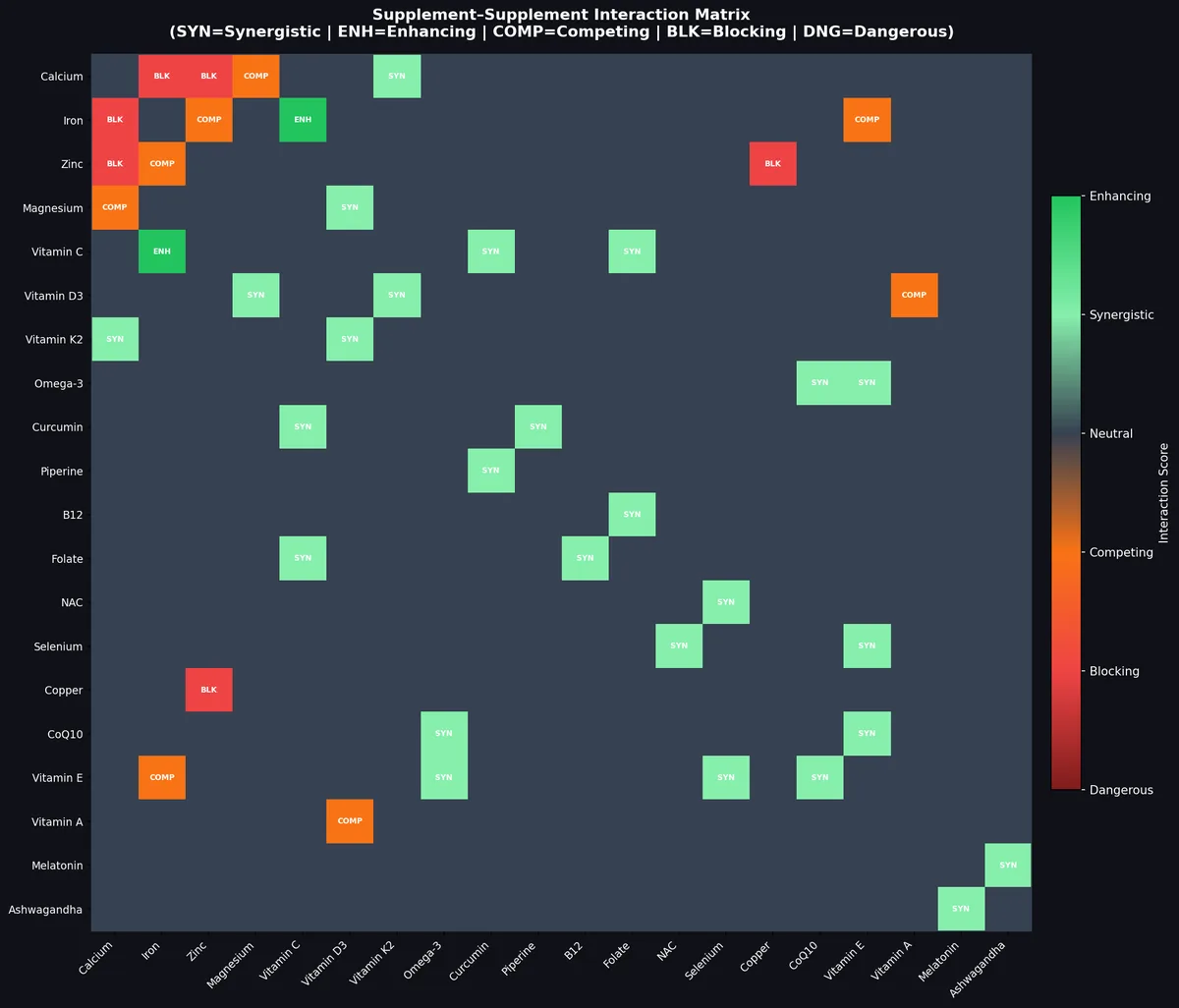
Quick Answer: The most important supplement interactions to know: Calcium blocks Iron and Zinc absorption (separate by 2+ hours). Zinc long-term depletes Copper (co-supplement 1-2mg Cu). Vitamin C dramatically enhances Iron absorption (always take together). D3 + K2 + Magnesium is a powerful synergistic triad. Piperine + Curcumin is one of the strongest bioavailability enhancers in supplementation. High-dose Vitamin A antagonizes Vitamin D3. Never combine 5-HTP or St. John’s Wort with SSRIs.
The heatmap above maps interaction scores across 20 key supplements: green = synergistic/enhancing, orange = competing, red/dark red = blocking/dangerous.
How to Read This Database
Each interaction is classified into one of six categories:
| Category | Code | Meaning |
|---|---|---|
| Synergistic | SYN | Both supplements enhance each other’s effect or absorption — take together |
| Enhancing | ENH | One supplement significantly boosts another’s bioavailability — take together |
| Neutral | — | No meaningful interaction at normal doses |
| Competing | COMP | Both reduce each other’s absorption; separate by 1–2 hours |
| Blocking | BLK | One significantly suppresses absorption of the other; separate by 2+ hours |
| Dangerous | DNG | Combination creates real risk of toxicity, adverse event, or drug interaction |
Category 1: Synergistic Combinations — Take These Together
These pairs work better together than apart. The synergy is supported by clinical evidence or well-established biochemical mechanisms.
D3 + K2 + Magnesium: The Triad
This is the most important three-way synergy in supplementation.
- Vitamin D3 increases calcium absorption from the gut. Without K2, that calcium can deposit in arteries rather than bone. [1]
- Vitamin K2 (MK-7) activates osteocalcin and Matrix Gla Protein (MGP), directing calcium to bone and away from soft tissue calcification.
- Magnesium is required to convert Vitamin D3 into its active form (calcitriol). Without adequate magnesium, Vitamin D supplementation can actually become ineffective or even create a magnesium deficiency. [2]
Stack: D3 (2,000–5,000 IU) + K2 MK-7 (100–200 mcg) + Magnesium Glycinate (300–400 mg) — all with dinner.
Curcumin + Piperine: Bioavailability 20x
Curcumin has poor oral bioavailability in standard form. A landmark 1998 study found that adding 20mg of piperine (the active compound in black pepper) increased curcumin bioavailability by 2,000% in humans. [3]
The mechanism: piperine inhibits intestinal glucuronidation (the process that eliminates curcumin before it reaches systemic circulation) and also inhibits CYP3A4 metabolism in the liver.
Important caveat: piperine also increases absorption of many drugs. If you’re on medications metabolized by CYP3A4 (many statins, immunosuppressants, certain antibiotics), check with your prescriber.
Stack: Curcumin (500–1,000 mg) + Piperine (20 mg) with a fatty evening meal.
Vitamin C + Iron: The Absorption Amplifier
Vitamin C converts ferric iron (Fe³⁺) to ferrous iron (Fe²⁺), which is the form absorbed through the DMT-1 transporter. This can increase non-heme iron absorption by 2–4x. [4]
This is one of the most consistently replicated nutrient synergies. If you’re treating or preventing iron deficiency, always take iron with 200–500mg of Vitamin C.
Stack: Iron bisglycinate (25–36 mg) + Vitamin C (250–500 mg) — midday, away from calcium.
NAC + Selenium: Glutathione Support
N-Acetyl Cysteine (NAC) provides cysteine, the rate-limiting amino acid for glutathione synthesis. Selenium is required for glutathione peroxidase (GPx), the enzyme family that uses glutathione to neutralize peroxides. These two nutrients work on complementary points of the same pathway. [5]
Stack: NAC (600–900 mg) + Selenium (100–200 mcg) — morning.
Omega-3 + Vitamin E: Oxidation Protection
Polyunsaturated fatty acids (EPA and DHA) are highly susceptible to oxidative rancidity. Vitamin E (mixed tocopherols) acts as a lipid-soluble antioxidant that protects omega-3s from oxidizing both in the bottle and in the body. This isn’t just theoretical — rancid fish oil has been shown in some studies to be pro-inflammatory rather than anti-inflammatory. [6]
Stack: Fish oil (1–3g EPA+DHA) + Vitamin E (200 IU mixed tocopherols) — morning with food.
B12 + Folate: The Methylation Pair
Methyl-B12 and L-methylfolate are interdependent in the methionine cycle. B12 is required to regenerate tetrahydrofolate (THF) from 5-methyltetrahydrofolate. Without adequate B12, folate gets “trapped” in a form that can’t be used — this is called the “methyl trap.” [7]
For MTHFR variant carriers (common — 40-60% of people carry one variant), getting both methylated forms is especially important.
Stack: Methyl-B12 (1,000 mcg) + L-Methylfolate (400–800 mcg) — morning.
Zinc + Vitamin A: Immune and Vision Synergy
Zinc is required for the synthesis of retinol-binding protein, which transports Vitamin A in the blood. Zinc deficiency directly impairs Vitamin A status even when Vitamin A intake is adequate. Conversely, adequate Vitamin A supports zinc-dependent immune functions. [8]
CoQ10 + PQQ: Mitochondrial Biogenesis
CoQ10 supports mitochondrial electron transport chain function. PQQ (Pyrroloquinoline quinone) stimulates mitochondrial biogenesis — the creation of new mitochondria. Together they support both quality and quantity of mitochondria.
Stack: CoQ10 (100–200 mg, ubiquinol form) + PQQ (10–20 mg) — morning with fat.
Category 2: Competing Interactions — Separate by 1–2 Hours
These pairs don’t block each other entirely but meaningfully reduce each other’s absorption when taken together.
Calcium + Magnesium
Both are divalent cations that share absorption pathways. At high doses, calcium supplementation can reduce magnesium absorption and vice versa. The clinical significance is most pronounced when doses are high (>500mg calcium, >200mg magnesium). At moderate doses taken together, the effect is mild. [9]
Practical rule: If you take high-dose calcium (1,000mg+), separate magnesium by 2+ hours.
Zinc + Iron
Both compete for the DMT-1 intestinal transporter. At a molar ratio of Zn:Fe above 1:1, zinc begins to meaningfully inhibit iron absorption, and vice versa. [10]
Practical rule: Take iron at midday, zinc in the morning.
Iron + EGCG (Green Tea Extract)
Polyphenols — including EGCG, quercetin, and tea tannins — form insoluble complexes with iron, blocking absorption. Green tea extract taken within 1–2 hours of iron can reduce absorption by 40–75%. [11]
Category 3: Blocking Interactions — Separate by 2+ Hours
These pairs have significant, well-documented absorption antagonism.
Calcium + Iron: The Most Common Hidden Deficiency Creator
High-dose calcium can meaningfully suppress iron absorption from the same meal. The Hallberg 1991 study showed a clear, dose-related reduction in non-heme iron absorption as calcium dose increased, with substantial inhibition in the 300–600 mg Ca range. More recent research has qualified these findings — the long-term (whole-diet) effect may be smaller than single-meal studies suggest — but for people actively treating iron deficiency, co-ingesting a calcium supplement with iron is still worth avoiding. [12]
This is one of the underappreciated causes of iron deficiency in women who take a calcium supplement daily alongside an iron supplement in the same dosing window.
Rule: Never take calcium and iron in the same 2-hour window.
Calcium + Zinc
Similar mechanism to calcium + iron. Divalent cation competition. Separate by at least 2 hours.
Zinc + Copper (Long-Term)
Zinc doesn’t acutely block copper absorption in the way calcium blocks iron — it’s a chronic effect. High-dose zinc (>40mg/day) induces metallothionein in intestinal cells, which preferentially sequesters copper. Over months, this can create symptomatic copper deficiency. [13]
Signs of zinc-induced copper deficiency: Anemia that doesn’t respond to iron, neutropenia, neurological symptoms.
Rule: If taking >25mg zinc daily long-term, supplement 1–2mg copper (not in the same meal — copper and zinc also compete modestly).
Category 4: Dangerous Interactions — Avoid These Combinations
High-Dose Vitamin A + Vitamin D3
At physiological doses, vitamins A and D work synergistically. At high doses (Vitamin A >10,000 IU/day supplementally), Vitamin A antagonizes Vitamin D receptor (VDR) activation, reducing D3’s anti-cancer, immune, and bone effects. [14]
Rule: If supplementing D3 seriously (3,000+ IU/day), keep supplemental preformed Vitamin A (retinol) under 3,000 IU. Beta-carotene (provitamin A) does not carry this risk.
5-HTP + SSRIs or MAOIs
5-Hydroxytryptophan is a direct serotonin precursor. Combining with serotonergic drugs (SSRIs, SNRIs, MAOIs) risks serotonin syndrome — a potentially life-threatening condition characterized by hyperthermia, agitation, tremor, and autonomic instability.
Rule: Do not take 5-HTP, St. John’s Wort, or SAMe with any serotonergic medication without medical supervision.
St. John’s Wort + Multiple Medications
St. John’s Wort is a potent inducer of CYP3A4 and P-glycoprotein. It significantly reduces blood levels of:
- Oral contraceptives (can cause contraceptive failure)
- Antiretrovirals (HIV medications)
- Cyclosporine (transplant rejection risk)
- Warfarin (reduced anticoagulation)
- Many statins, antidepressants, antiepileptics
Rule: Treat St. John’s Wort as a drug interaction risk equivalent to a pharmaceutical CYP3A4 inducer.
Fat-Soluble Vitamin Mega-Dosing
Taking high-dose A + D + E + K together without testing creates unpredictable accumulation. Unlike water-solubles, these store in tissue:
- Vitamin A toxicity (hypervitaminosis A): >25,000 IU/day over months causes liver damage, intracranial pressure, teratogenicity
- Vitamin D toxicity: >60,000 IU/day over weeks causes hypercalcemia, kidney stones, soft tissue calcification
The Complete Interaction Matrix: Key Pairs Summary
| Supplement A | Supplement B | Interaction | Action |
|---|---|---|---|
| Vitamin D3 | Vitamin K2 | Synergistic | Always pair |
| Vitamin D3 | Magnesium | Synergistic | Always pair |
| Vitamin D3 | Vitamin A (high dose) | Antagonistic | Cap retinol <3,000 IU |
| Vitamin C | Iron | Enhancing | Always pair |
| Curcumin | Piperine | Enhancing | Always pair (20mg BioPerine) |
| Omega-3 | Vitamin E | Enhancing | Pair in same meal |
| B12 | Folate | Synergistic | Methylated forms preferred |
| NAC | Selenium | Synergistic | Morning stack |
| CoQ10 | Omega-3 | Synergistic | Cardiovascular stack |
| Zinc | Copper | Blocking (chronic) | Supplement Cu if Zn >25mg/day |
| Calcium | Iron | Blocking | Separate by 2h minimum |
| Calcium | Zinc | Blocking | Separate by 2h minimum |
| Calcium | Magnesium | Competing | Separate if high dose |
| Zinc | Iron | Competing | Separate by 2h |
| Iron | EGCG/Tea | Competing | Separate by 2h |
| Iron | Vitamin C | Enhancing | Take together |
| Magnesium | Vitamin D3 | Synergistic | Always pair |
| 5-HTP | SSRIs/MAOIs | Dangerous | Never combine |
| St. John’s Wort | Most Rx drugs | Dangerous | Contraindicated |
| Vitamin A (high) | Vitamin D3 | Antagonistic | Limit retinol supplementation |
| Melatonin | Ashwagandha | Synergistic | Sleep stack |
| Selenium | Vitamin E | Synergistic | Antioxidant pair |
Synergistic Stacks Worth Building
Beyond individual pairs, several well-researched multi-supplement stacks produce additive or synergistic benefits:
The Cardiovascular Stack
Omega-3 (3g EPA+DHA) + CoQ10 (200mg ubiquinol) + Magnesium Taurate (400mg) + Vitamin K2 (200mcg) + Vitamin E (200 IU mixed tocopherols)
Rationale: Omega-3 and CoQ10 independently support mitochondrial function and cardiac energy. K2 prevents vascular calcification. Magnesium taurate supports heart rhythm (taurine has membrane-stabilizing effects). Vitamin E protects omega-3 from oxidation and provides independent cardiovascular antioxidant activity.
The Cognitive Stack
Lion’s Mane (500mg) + Bacopa (300mg) + Omega-3 (2g DHA-rich) + Magnesium Threonate (144mg elemental) + Phosphatidylserine (300mg)
Rationale: Lion’s Mane stimulates nerve growth factor (NGF). Bacopa enhances memory consolidation (though takes 8–12 weeks). DHA is the structural fatty acid of the brain. Magnesium threonate is the only form that meaningfully increases brain magnesium. Phosphatidylserine is the most evidence-backed cognitive supplement, with FDA-qualified health claim.
The Immune Foundation Stack
Vitamin D3 (4,000 IU) + K2 (100mcg) + Zinc (25mg) + Selenium (100mcg) + Vitamin C (1,000mg split AM/PM) + Elderberry (600mg)
Rationale: Vitamin D3 modulates innate and adaptive immunity. Zinc is required for T-cell development and function. Selenium is essential for glutathione peroxidase and antiviral response. Vitamin C concentrates in white blood cells at 50–100x plasma levels. All work on complementary immune pathways.
The Blood Sugar Balance Stack
Berberine (500mg 3x/day) + Magnesium (400mg) + Chromium Picolinate (200mcg) + Alpha Lipoic Acid R-form (300mg) + Cinnamon Extract (500mg)
Rationale: Berberine activates AMPK (similar to metformin). Magnesium deficiency causes insulin resistance. Chromium enhances insulin receptor sensitivity. R-ALA improves GLUT4 translocation. Cinnamon polyphenols modulate glucose transporter activity.
The Sleep Architecture Stack
Magnesium Glycinate (400mg) + L-Theanine (200mg) + Ashwagandha KSM-66 (300mg) + Glycine (3g) + Apigenin (50mg) + Melatonin (0.5–1mg)
Rationale: Magnesium activates GABA receptors. L-Theanine promotes alpha brainwave activity. Ashwagandha lowers cortisol. Glycine lowers core body temperature (a trigger for sleep onset). Apigenin has mild GABA-A modulating activity. Melatonin signals circadian phase. Each targets a different sleep mechanism — no redundancy.
Herb-Drug Interactions: The Overlooked Category
Most supplement interaction discussions focus on vitamins and minerals. Herbal supplements carry some of the most significant interaction risks — particularly through CYP450 enzyme modulation:
| Herb | Interaction Mechanism | Affected Drugs |
|---|---|---|
| St. John’s Wort | CYP3A4 inducer (strong) | Oral contraceptives, antiretrovirals, cyclosporine, warfarin, many antidepressants |
| Ginkgo Biloba | Antiplatelet; CYP2C9 modulation | Warfarin, aspirin, NSAIDs; increased bleeding risk |
| Garlic Extract | Antiplatelet; CYP2E1 modulation | Warfarin, antiplatelet drugs |
| Milk Thistle | CYP3A4 inhibitor (mild) | Statins, immunosuppressants |
| Piperine (black pepper extract) | CYP3A4 and P-gp inhibitor | Many drugs metabolized by CYP3A4 |
| Valerian | CNS depressant synergy | Benzodiazepines, opioids, sedatives |
| Kava | CYP1A2, CYP2D6, CYP3A4 inhibitor | Multiple drug classes; hepatotoxicity risk alone |
| Berberine | P-gp inhibitor; CYP2D6, 3A4 | Many drugs; particularly relevant with Metformin (additive hypoglycemia risk) |
| Ashwagandha | Thyroid stimulation | Thyroid medications; check TSH if using |
| Melatonin | CYP1A2 substrate | Fluvoxamine, caffeine (increase melatonin levels) |
Building a Conflict-Free Stack
Step 1: Identify your blockers
Iron and calcium cannot coexist in the same dosing window. If you take both, one goes in the morning and one at midday.
Step 2: Pair your synergists
D3 + K2 + Magnesium should always be in the same dose. Curcumin always with piperine. Iron always with Vitamin C.
Step 3: Check copper when zinc is high
If your stack includes >25mg zinc daily, add 1–2mg copper — but in a different meal.
Step 4: Separate competing minerals
Zinc, iron, calcium, and magnesium all compete. Spread them across 2–3 windows throughout the day.
Step 5: Red-flag medications
If you take any prescription drug, check St. John’s Wort, piperine (CYP3A4), and fat-soluble vitamins specifically. These have the highest drug-supplement interaction rates.
Frequently Asked Questions
Does taking zinc and copper together cancel them out?
Slightly, yes — zinc and copper do compete for absorption. The standard recommendation is to take them in different meals. However, the bigger concern is chronic zinc without copper: over months, high zinc induces metallothionein that sequesters copper. Add 1–2mg copper if taking more than 25mg zinc daily for extended periods.
Is it safe to take vitamin D3 and vitamin A together?
At physiological doses, yes. The problem is high-dose supplemental vitamin A (retinol) — doses above 10,000 IU/day can antagonize vitamin D receptor function. Stick to beta-carotene as your vitamin A source or keep supplemental retinol below 3,000 IU if you’re taking therapeutic D3 doses.
Do herbal supplements interact with each other?
Yes, significantly. Ashwagandha, Rhodiola, and Holy Basil are all adaptogens that modulate cortisol — stacking all three isn’t dangerous but may produce diminishing returns. More critically, botanicals like St. John’s Wort, Ginkgo, and high-dose garlic extract can interact with pharmaceutical drugs. Always check herb-drug interactions separately.
Can I take magnesium and calcium together?
At low to moderate doses (300mg magnesium, 500mg calcium), co-administration is fine. At high doses (especially for calcium supplementation for osteoporosis), separate them by 2 hours to optimize magnesium absorption.
What’s the best free resource to check supplement interactions?
The NIH Office of Dietary Supplements (ods.od.nih.gov) publishes individual fact sheets with interaction data. Examine.com and ConsumerLab.com also maintain interaction databases. For drug-supplement interactions specifically, Natural Medicines Database (subscription) is the clinical gold standard.
Related Articles
- Supplement Timing Guide: The Complete Daily Stack Schedule
- Supplement Forms Guide: Glycinate vs Citrate vs Oxide
- Lab Value to Supplement Decision Tree: 20 Biomarkers Decoded
- Supplement Safety Ceiling Database: Upper Limits and Toxicity Data
Sources
1. Schurgers LJ, Vermeer C. Determination of phylloquinone and menaquinones in food. Haemostasis. 2000;30(6):298-307.
2. Uwitonze AM, Razzaque MS. Role of Magnesium in Vitamin D Activation and Function. J Am Osteopath Assoc. 2018;118(3):181-189.
3. Shoba G, Joy D, Joseph T, et al. Influence of piperine on the pharmacokinetics of curcumin in animals and human volunteers. Planta Med. 1998;64(4):353-356.
4. Hallberg L, Brune M, Rossander L. The role of vitamin C in iron absorption. Int J Vitam Nutr Res Suppl. 1989;30:103-108.
5. Dröge W, Breitkreutz R. Glutathione and immune function. Proc Nutr Soc. 2000;59(4):595-600.
6. Albert BB, Cameron-Smith D, Hofman PL, Cutfield WS. Oxidation of marine omega-3 supplements and human health. Biomed Res Int. 2013;2013:464921.
7. Scott JM. Folate and vitamin B12. Proc Nutr Soc. 1999;58(2):441-448.
8. Salgueiro MJ, Zubillaga M, Lysionek A, et al. Zinc as an essential micronutrient: a review. Nutr Res. 2000;20(5):737-755.
9. Sabatier M, Arnaud MJ, Kastenmayer P, et al. Meal effect on magnesium bioavailability from mineral water in healthy women. Am J Clin Nutr. 2002;75(1):65-71.
10. Sandström B. Micronutrient interactions: effects on absorption and bioavailability. Br J Nutr. 2001;85 Suppl 2:S181-185.
11. Zijp IM, Korver O, Tijburg LB. Effect of tea and other dietary factors on iron absorption. Crit Rev Food Sci Nutr. 2000;40(5):371-398.
12. Hallberg L, Brune M, Erlandsson M, et al. Calcium: effect of different amounts on nonheme- and heme-iron absorption in humans. Am J Clin Nutr. 1991;53(1):112-119.
13. Olivares M, Uauy R. Copper as an essential nutrient. Am J Clin Nutr. 1996;63(5):791S-796S.
14. Johansson S, Melhus H. Vitamin A antagonizes calcium response to vitamin D in man. J Bone Miner Res. 2001;16(10):1899-1905.
- Ma et al. (2025). Effect of serum magnesium on mortality in intensive care unit patients with heart failure: a retrospective analysis …. Zhonghua wei zhong bing ji jiu yi xue. PMID: [41500689
- Mitsuboshi et al. (2026). Laxative use and acute kidney injury risk: Analysis of a Japanese hospital-based database. The Journal of pharmacology and experimental therapeutics. PMID: 41806409
- Daigle et al. (2026). Leveraging long-read assemblies and machine learning to enhance short-read transposable element detection and genotyping. Genetics. PMID: 41996583
- Luo et al. (2026). Serum iron is associated with the prognosis in sepsis based on a large-scale database. BMC infectious diseases. PMID: 41772469
- He et al. (2026). High-pathogenicity island enhances NDM-5 activity and drives global spread of Escherichia coli ST410. The ISME journal. PMID: 41968391
- Mao et al. (2026). Neuroprotective Impact of Magnesium Sulfate on Mortality in Sepsis-Associated Encephalopathy: A Propensity-Matched An…. CNS & neurological disorders drug targets. PMID: 41833045
AI-Assisted Content Disclosure
This interaction database was researched and drafted with AI assistance and reviewed for accuracy. Quantitative effect sizes (e.g., percent absorption changes) reflect specific study conditions and dosages and may not apply identically to every individual or product. Supplement–drug interactions in particular are incompletely characterized in the literature and can be product- and dose-specific. Nothing here is medical advice. Check with a pharmacist or physician before combining supplements with prescription medications, especially blood thinners, antidepressants, thyroid medication, transplant drugs, and antiretrovirals.


Leave a Reply