
Quick Answer: Calcium carbonate and calcium citrate are the most evidence-backed forms — citrate absorbs better without food and matters most for people with low stomach acid. Women over 50 should aim for 1,200 mg/day from food plus supplements combined, but splitting doses and pairing with vitamin D3 and K2 significantly improves absorption and reduces kidney stone risk.

Calcium is the most abundant mineral in the human body, comprising about 99% of your bones and teeth. Yet calcium supplementation remains one of the most misunderstood topics in health — plagued by debates over form, timing, co-factors, and the contentious relationship with kidney stones and cardiovascular risk.
This guide cuts through the noise with evidence-based guidance on the best calcium supplement forms, dosing strategies, and the special considerations for women over 50.
Why Calcium Supplementation Is Complicated
Getting enough calcium sounds simple — bones need calcium. But the reality involves a cascade of interacting factors: absorption efficiency, vitamin D status, magnesium levels, vitamin K2, gastric acid production, age-related changes, and the ongoing controversy over whether supplemental calcium increases cardiovascular or kidney stone risk.
The 2010 meta-analysis in the British Medical Journal (Bolland et al.) alarmed many by suggesting calcium supplements raised heart attack risk by 27–31%. Follow-up research has been mixed, and most large reviews since have not confirmed the cardiovascular signal when calcium is taken with vitamin D and within recommended amounts. However, the debate has prompted important refinements in how we think about supplementation.
Calcium Supplement Forms: What Matters
Calcium Carbonate
The most widely used form. Each tablet delivers 40% elemental calcium by weight, making it the most concentrated option. However, calcium carbonate requires stomach acid for optimal absorption and should be taken with food.
Best for: Most adults who eat regular meals and have normal stomach acid production.
Drawbacks: Can cause constipation and bloating. Poor choice if you take acid-reducing medications (PPIs, H2 blockers) or have achlorhydria.
Calcium Citrate
Contains 21% elemental calcium, but doesn’t require stomach acid. Can be taken with or without food.
Best for: Adults over 60, anyone taking PPIs or antacids, those with inflammatory bowel disease or absorption issues.
Drawbacks: Larger pill sizes and more pills needed per dose, typically more expensive.
Calcium Malate and Calcium Glycinate
These chelated forms offer good bioavailability and tend to be gentler on digestion. Calcium glycinate in particular may cause less GI distress than carbonate.
Best for: People who experience digestive discomfort with other forms.
Calcium Phosphate (Tricalcium Phosphate)
Moderate absorption, less constipating than carbonate, and commonly used in fortified foods. Not a common standalone supplement but is found in many multivitamins.
Forms to Approach with Caution
- Bone meal, oyster shell, and dolomite: Older natural sources that may contain lead and other heavy metals. Avoid.
- Calcium from coral: Not recommended due to environmental concerns and potential contamination.
How Much Calcium Do You Actually Need?
Recommended Dietary Allowances (RDA) by age:
| Age Group | RDA | |—|—| | Adults 19–50 | 1,000 mg/day | | Men 51–70 | 1,000 mg/day | | Women 51–70 | 1,200 mg/day | | Adults 71+ | 1,200 mg/day | | Pregnant/Lactating women | 1,000 mg/day |
The RDA includes calcium from all sources — food, fortified foods, and supplements combined. Most Americans consume 700–1,000 mg daily from food, meaning many women over 50 are meaningfully short.
Tolerable Upper Intake Level (UL): 2,000–2,500 mg/day. Chronically exceeding the UL is associated with hypercalcemia, kidney stones, and possibly cardiovascular effects.
Timing and Absorption: The Critical Details
Split Your Doses
The body can absorb only about 500 mg of calcium at a time. Taking more than that in a single dose simply wastes the excess. If you need 1,000 mg supplemental calcium daily, take two 500 mg doses — one in the morning, one in the evening.
Take Calcium Carbonate With Food
Calcium carbonate needs gastric acid. Take it within 30 minutes of a meal. Calcium citrate can be taken any time.
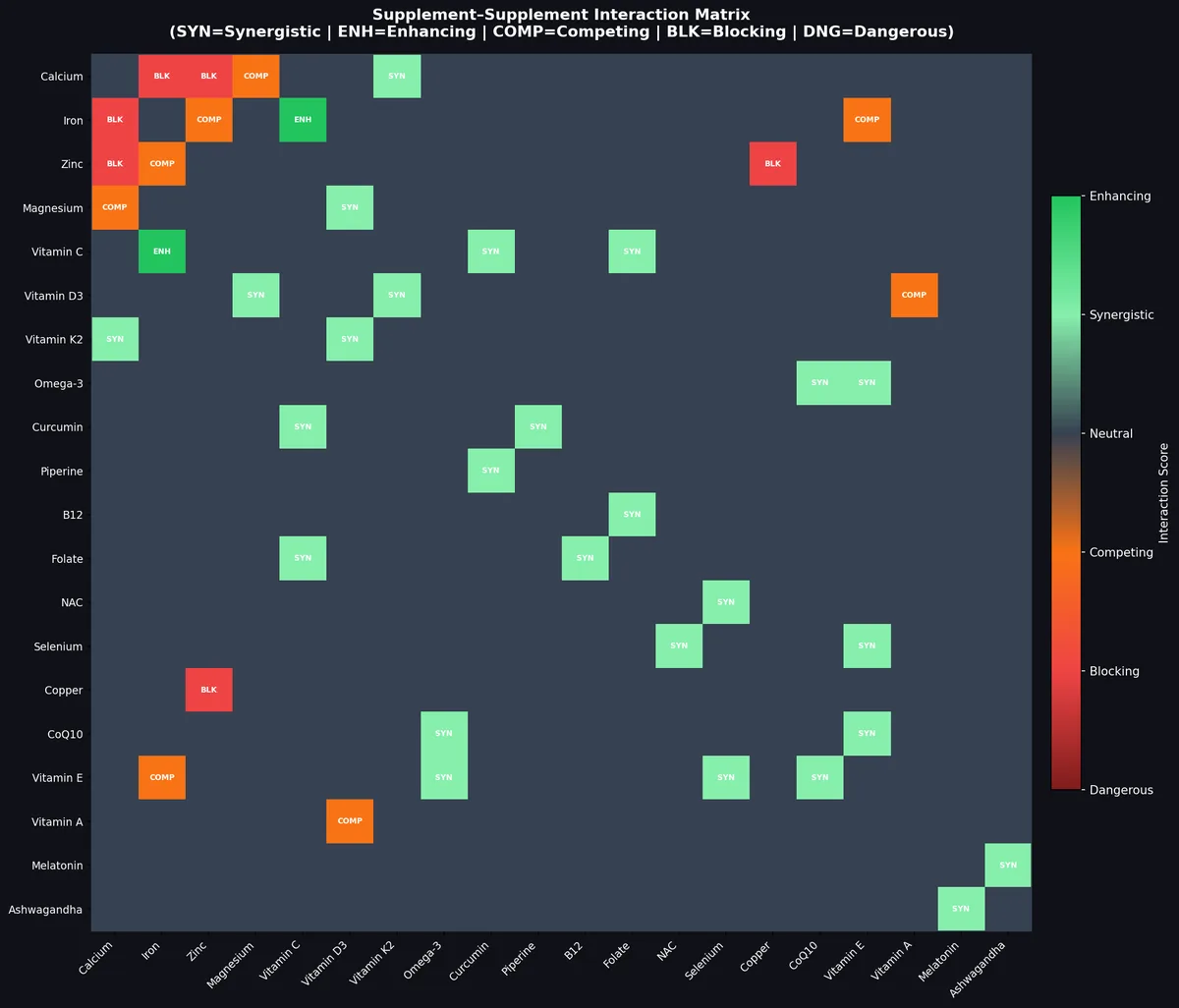
Don’t Take Calcium With Iron Supplements
Calcium significantly inhibits iron absorption. Separate calcium and iron supplements by at least 2 hours.
Magnesium and Calcium Compete
High-dose supplemental calcium can interfere with magnesium absorption. Many integrative practitioners recommend a 2:1 calcium-to-magnesium ratio, or taking magnesium separately in the evening.
Women Over 50: The Bone Health Priority
After menopause, estrogen levels drop sharply, and bone resorption accelerates. Women can lose up to 20% of bone density in the 5–7 years post-menopause. This is the primary reason women over 50 have a higher RDA for calcium.
Key considerations:
Vitamin D is essential. Without adequate vitamin D3 (800–2,000 IU/day for most adults), calcium absorption drops dramatically. Many women over 50 are D-deficient. Test your 25(OH)D levels. The optimal range for bone health is 40–60 ng/mL.
Vitamin K2 directs calcium to bone. Vitamin K2 (specifically MK-7 form, 90–200 mcg/day) activates osteocalcin and matrix GLA protein (MGP), proteins that help shuttle calcium into bone and away from arteries. There is growing evidence that calcium supplementation without K2 may increase arterial calcification risk. Consider a combined D3/K2 supplement.
Magnesium is underappreciated. Magnesium plays a role in vitamin D metabolism and directly in bone mineralization. Many older women are borderline deficient. 300–400 mg/day of magnesium glycinate or malate is reasonable.
Resistance training matters more than supplements alone. Weight-bearing exercise stimulates bone remodeling and is the most effective long-term strategy for preventing osteoporosis.
The Kidney Stone Question: What the Evidence Actually Shows
The fear of kidney stones from calcium supplementation is real but context-dependent.
The most common kidney stones are calcium oxalate stones, formed when calcium and oxalate bind in the kidneys. Here’s the paradox: dietary calcium actually reduces kidney stone risk, because it binds oxalate in the gut before it reaches the kidneys. This effect is reduced when calcium supplements are taken apart from meals.
The risk with supplements is primarily timing:
- Taking calcium supplements with meals reduces oxalate absorption and lowers stone risk
- Taking calcium supplements away from food means calcium arrives in the kidneys with more urinary oxalate, increasing risk
A major 2018 systematic review in the Journal of Urology found that the stone risk from supplemental calcium is significantly lower when taken with food. The absolute excess risk is also quite small — roughly 17% relative increase seen in some studies translates to a small number of additional cases per 10,000 women per year.
People at higher kidney stone risk should:
- Stay well-hydrated (aim for 2+ liters of urine per day)
- Always take calcium supplements with meals
- Reduce dietary oxalate (spinach, nuts, chocolate, tea)
- Avoid exceeding 1,000 mg/day supplemental calcium
- Consult a nephrologist if they have a history of calcium oxalate stones
The Cardiovascular Controversy Revisited
The Bolland 2010 meta-analysis that triggered concerns about calcium supplements and heart attacks has been reanalyzed multiple times. Key follow-up findings:
- The Women’s Health Initiative (WHI) study found no significant cardiovascular increase when calcium was taken with vitamin D
- A 2020 meta-analysis in JAMA Internal Medicine did not find calcium supplementation significantly increased MI risk when taken within recommended doses
- The hypothesis is that calcium carbonate taken without food may cause acute spikes in serum calcium (“calcium waves”) that promote arterial calcification
The practical takeaway: Avoid megadosing calcium, take it with food, ensure K2 status is adequate, and don’t rely on supplements to compensate for a calcium-poor diet.
Calcium from Food: The Gold Standard
Dietary calcium comes packaged with cofactors, tends to enter the bloodstream more gradually, and doesn’t appear to carry the same risk as isolated supplements. High-calcium foods include:
| Food | Calcium (mg) | |—|—| | Whole milk (1 cup) | ~300 | | Plain yogurt (1 cup) | ~415 | | Cheddar cheese (1.5 oz) | ~307 | | Sardines, canned (3 oz) | ~325 | | Tofu, calcium-set (½ cup) | ~350 | | Kale, cooked (1 cup) | ~177 | | Bok choy, cooked (1 cup) | ~158 | | Almonds (1 oz) | ~76 | | Fortified OJ (1 cup) | ~350 |
What to Look for When Buying Calcium Supplements
Third-party testing: Look for USP Verified, NSF Certified, or ConsumerLab tested products. This ensures the label’s calcium content is accurate and heavy metals are within safe limits.
Elemental calcium, not compound weight: Labels often list the total compound weight (e.g., 1,000 mg calcium carbonate), but the elemental calcium is 40% of that = 400 mg. Check the supplement facts panel for “elemental calcium.”
Avoid excessive filler ingredients in cheaper products. Simple formulations are preferable.
D3/K2 combo products are increasingly popular and convenient for those who want all three in one capsule.
Key Takeaways
- Calcium citrate is the most versatile form — it absorbs well without food and is best for those over 60 or on acid-reducers
- Calcium carbonate is effective and affordable but must be taken with food
- Split doses: Never take more than 500 mg calcium at one time
- Women over 50 need 1,200 mg/day total; supplements fill the gap above dietary intake
- Vitamin D3 + K2 dramatically improves calcium’s effectiveness and safety profile
- Kidney stone risk from supplements is mainly a timing issue — take calcium with meals
- Don’t exceed 2,000 mg/day total calcium from all sources
- Food-first approach remains preferred; supplement to close genuine gaps
Frequently Asked Questions
What is the best form of calcium supplement to take?
Calcium citrate is the best choice for most adults over 50, those on acid-lowering medications, and anyone with digestive issues. Calcium carbonate is effective for younger, healthy adults who take it with food and have normal stomach acid.
Should I take calcium and vitamin D together?
Yes. Vitamin D3 is required for calcium absorption in the gut. Without sufficient D3 (at least 800 IU/day, ideally 1,000–2,000 IU/day), much of your supplemental calcium is poorly absorbed. Many products combine both.
Can calcium supplements cause kidney stones?
The risk exists but is largely timing-dependent. Taking calcium supplements with meals reduces oxalate absorption and minimizes kidney stone risk. Those with a history of calcium oxalate stones should discuss supplementation with their doctor.
How much calcium should a woman over 60 take daily?
The RDA is 1,200 mg/day total from food and supplements. Most women get 700–900 mg from diet, leaving a 300–500 mg gap that can be supplemented safely. Avoid exceeding 500 mg in a single dose.
Is it safe to take calcium supplements every day?
Yes, within the recommended range. Staying below 1,000–1,200 mg supplemental calcium per day, taken with food and paired with D3 and K2, is considered safe for most adults.
Does vitamin K2 really matter with calcium?
Emerging evidence suggests K2 (especially MK-7) helps direct calcium to bones rather than arteries. It activates MGP, a protein that prevents vascular calcification. While not definitively proven in large RCTs, the safety profile is excellent and the mechanistic evidence is strong enough that many practitioners recommend 90–200 mcg MK-7 with calcium and D3.
Sources
- Bolland MJ, et al. (2010). Effect of calcium supplements on risk of myocardial infarction and cardiovascular events. BMJ, 341:c3691.
- Jackson RD, et al. (2006). Calcium plus vitamin D supplementation and the risk of fractures. NEJM, 354(7):669–683.
- Curhan GC, et al. (1997). Comparison of dietary calcium with supplemental calcium in the prevention of kidney stones. Ann Intern Med, 126(7):497–504.
- Weaver CM, et al. (2016). Calcium plus vitamin D supplementation and risk of fractures: an updated meta-analysis. Osteoporosis Int, 27(1):367–376.
- Maresz K. (2015). Proper calcium use: vitamin K2 as a promoter of bone and cardiovascular health. Integrative Medicine, 14(1):34–39.
- Office of Dietary Supplements – NIH. (2023). Calcium Fact Sheet for Health Professionals.
- Harvey NC, et al. (2017). Calcium supplementation and cardiovascular risk. JAMA Intern Med, 177(7):1031.


Leave a Reply